CONGENITAL ALOPECIA AS AN EXPRESSION OF ATAVISM
By JAMES NEVINS HYDE, M.D.
UNDER the several titles, Alopecia, Congenital Hypotrichiasis, Universal Congenital Atrichia, and Congenital Alopecia Areata, have been described as a group of rare cases in which the symptoms, presumably originating from different causes, have presented a suggestive similarity. The obscurity, however, in which the origin and later history of total absence, or scanty growth of hair at birth have been shrouded, is noted by several writers. The following named conditions are chiefly those to which attention has been directed in the consideration of this subject:
(1) Complete and universal absence of hair at birth, not succeeded later in life by a pilary growth. This is believed to be an intra-uterine atrichia, due to failure of development of the hair-pouches.
(2) Universal congenital hypotrichiasis, in which at birth hairs exist in all regions of the body, but later fail to be succeeded by filaments normal in length, vigor, color, and texture. Two sub-varieties of this condition have been recognized.
(a) The infant at birth is provided with the relatively long hair of most normal infants. This in due time falls and is replaced by a scanty down which later in life fails to ensure normal hirsute- ness of the scalp.
(b) After birth the infant fails to lose the temporary hair of the scalp which persists, but later develops merely a scanty or ill-developed pilary growth.
(3) Complete or partial absence of hair at birth in definitely circumscribed regions, such as the scalp, the brows, the pubes, or the axillæ.
Dubreuilh and Petges distinguish between the following forms of circumscribed congenital alopecia:
(A) Circumscribed nævic congenital alopecia, including cases where nævus lesions develop on plaques of alopecia; cases where a [p.30] nævus in process of involution leaves its relics on a similar plaque; and cases where, either in the immediate vicinity of, or in actual continuity with, a patch of alopecia a circumscribed nævus develops. In all cases there is an irregularly round or oval patch slightly projecting, often mamelonnated, at times darkly pigmented, and covered with a fine growth of downy hairs.
(B) Circumscribed congenital alopecia, due to arrested development of the skin, in which the plaques are small and situated near the posterior fontanelle, over the occiput, or over or near the median line; no downy hair is present nor are there evidences of cicatrix or atrophy.
(C) “Obstetrical” alopecia, characterized by irregularities of the zone affected with alopecia. The form of the patch is variable, the skin somewhat thin, unprovided with down and exhibiting no cicatrix. The patch is relatively large and situated on the frontal or fronto-parietal regions. These cases are supposed to be due to the action of the obstetrical forceps.
(D) “Sutural” alopecia, due to the enlargement of the cranial vault prior to the union of the fontanelles (hydrocephalus, etc.), the patches occurring in the region of the sutures, with adhesion to the deeper parts and irregular growth of hairs, few in number and disposed without order.
(4) Generalized or circumscribed absence of hair at birth, followed in later life by a normal hair-development. This condition is believed by writers to be due to pre-existing intra-uterine disease, or to such a disease seriously involving the hair-pouches at birth, resulting in a true alopecia, evidences of which may be wanting at the date of first examination by the physician. Thus some cases of congenital hair-absence are recorded as due to alopecia areata, to intra-uterine nervous shock, etc.
(5) Cases in which one or all of the anomalies cited above co-exist with anomalous conditions recognized in the teeth, nails, and other organs.
Under the title, Congenital Dyskeratoses. Lenglet has grouped many of the disorders named above and others (foetal ichthyosis, congenital ichthyosiform erythrodermia, palmar and plantar keratodermia, circumscribed and generalized atrophies, etc.) affecting what the French call the phanères of the integument. The types which for purposes of classification he has sought to establish, are
[p.31] chiefly distinguished by the behavior of the epitrichial layer after the birth of the infant; the layer in some cases, after abnormal persistence, seeming to assume a species of pseudo-autonomy; in other cases retaining a close relation to the deeper integumentary structure and profoundly influencing its evolution.
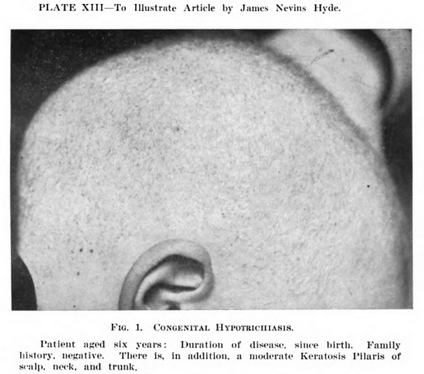
During the last twenty years, the clinical records of my associates and myself in both public and private practice have included a series of cases of congenital alopecia. In no one of these patients has the congenital absence of hair been absolutely complete. A patient most nearly presenting such an anomaly was exhibited at the Clinic in the year 1893. The subject was a female child, two and a half years old, which on first inspection seemed to be wholly destitute of hair. Careful scrutiny with a lens, however, detected over the scalp surface a very few points where slender downy hairs were produced in fine wisps. The larger number of cases coming under our observation have been those of patients who, from the hour of birth, exhibited either an exceedingly restricted area of hair-growth or, what was more common, a growth of hair duly covering the normal areas; the pilary filaments, none the less, being markedly deficient in length, vigor, and texture. (Fig. 1.)
Subjoined are notes of the case of a patient recently presented, where the departure from the normal standard lay along the line of a wider divergence from type than is commonly recognized:
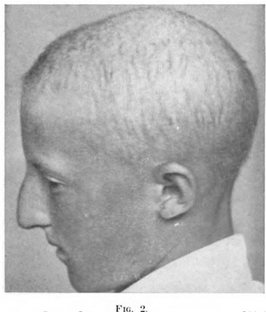
E. K., male, fourteen years of age, was presented by his parents for examination in June, 1908. The following data were communicated respecting his family history: his father’s father, aged 71, is living in sound health; his father’s mother died of paralysis in her seventy-first year; he has two uncles living in good health; one of these is the father of three children; he has also an aunt now living, in good health, the mother of a child.
On the mother’s side, a grandmother is living, aged 68; two uncles are living, none dead; one maternal aunt, living, is the mother of two healthy children. The mother’s father died of tuberculosis in his thirty-second year. No member of the family is known to have exhibited an abnormal feature at birth. There have been no intermarriages.
On physical inspection, the patient is found to present in general the usual aspect of bodily health. In the matter of nu- [p.32] trition, weight, stature, organs of sense, and muscular development, he is in correspondence with the average youth of his age. mental attainments are in no degree at fault. He has advanced with success to the second year of high school study. Puberty has been safely reached. The genitalia exhibit no signs of infantilism. The general hue of the patient’s skin is that of health, though the integument is the seat of a mild xerosis, most conspicuous over the face. Here and there over the surface of the body, in the regions where such phenomena are usually most pronounced, can be recognized a moderate degree of keratosis of the pilaris type.
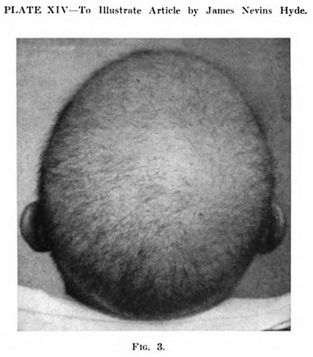
The scalp is normal in color and texture and is completely covered with scanty, short, stiff hairs pointed at the extremity and nonpigmented, averaging not more than a centimètre in length. This condition, without appreciable change, has existed since birth. A few dark-tinted hairs are visible at the inner margin of the brows. Similarly, a few scattered lashes can be recognized along the edges of the lids. There are no traces of a beard. Some rudimentary and lanugo hairs may be found at various points over the trunk and limbs.
The teeth are normal in number and color, though unusually separated, small, and notably peg-shaped. The frenum of the upper lip extends below the inferior border of the gum and is brought down between the separated central incisors.
The finger-nails are convexly curved to the point of exaggeration from side to side, and the nail-beds are readily exsanguinated under pressure. The toe-nails are distinctly thickened and transversally ridged.
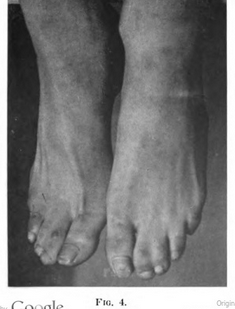
Between the first and second fingers, as also between the third and fourth fingers of both hands, is stretched a web which extends from the line of the metacarpophalangeal articulations about half- way to the distal extremities of the involved digits. These webs are constituted of skin and connective tissue. The second and third toes of both feet are united by a similar web which, however, in these organs practically extends throughout the length of the digits. with the effect of welding each couple into a single organ. A similar web, but not extending to a greater length than those between the webbed fingers, stretches between the third and fourth toes of both feet. Skiagraphic examination of the webs of both feet and hands gives negative results.
[p.33] An exostosis, of the size of an English walnut, springs from the external and posterior face of the os calcis of the left foot. A first examination suggests that there has been a line of cleavage between the tuberosity of the calcaneum and its anterior portion supporting the astragalus.
There is moderate and symmetrical enlargement of the thyroid gland. The pulse is 120 to the minute; but there is no exophthalmos, no tremor, and the Romberg test gives negative results.
I am indebted to Dr. James MacFarlane Winfield, of Brooklyn, for the following details respecting the similar condition of a patient under his observation:
“In 1899 Mr. A. C., age 35, consulted me for an eczematous condition of the skin of the flexor surfaces of the extremities, the inflammation being more marked about the elbows and knees. He stated that his skin had always given him trouble on account of “dryness” and when irritated, as by overheating or the presence of woolen under-clothing, he would be apt to have an eczematous outbreak. A condition of xerodermia had existed since birth. The patient only perspired in very hot weather and in the Turkish bath.
“S. P. The hairy development is markedly imperfect, there being none on the arms and legs, and only a few feeble lanugo hairs over the pubes and axillæ. Although the patient states that he is obliged to shave once or twice a week, upon the closest inspection no hairs can be seen on the face, the hair is so fine and light colored. The hair of the head is a fine and sparse lanugo, the scalp is covered but the hair grows slowly. The head resembles that of a six months old infant with slow hairy development. His mother states that at birth the scalp was covered with a fine down, which soon fell he remained completely bald until he was between seven and eight years old; then a few hairs grew on the scalp; at puberty the hairs developed merely to the condition described above. The first dentition was delayed until he was between three and four years of age; and when the teeth came in they were “small and weak,” dropping out and decaying before he was ten years old. The second dentition was normal as to time of eruption. He still has all of his teeth although some of them have been filled. They are peg-shaped and with large spaces between each tooth, resembling the setting of a dog’s teeth.
[p.34] “He is very myopic, being obliged to wear the strongest glasses obtainable: even then his vision is very imperfect.
“The middle, ring, and little fingers of both hands are joined with a web, the webbing extends up to the distal joint. The toes are similarly webbed. The finger and toe-nails are thin and friable. His ears are small and misshapen (no lobes).
“His general health has always been good: mentality unimpaired. There is no record of degeneracy in the ancestors of either parent; though his mother has a mild grade of xerodermia.”
Surveying the records of cases described as Congenital Alopecia, it is evident that the anomaly is rare, even in the list of rare anomalies of the skin and its appendages; and also, of still greater rarity when evidenced by an absolute and general failure of pilary development at birth, persisting through life. Many of the published observations of this anomaly are lacking in details of special im- portance. Dentists and dental surgeons seem to have given scanty attention to the condition of the hair and nails: the general practitioner, on the other hand, has often neglected to describe the dental condition. Of fifty-six records of so-called congenital alopecia, where the sex of the subject is given, it appears that thirty-eight were males and eighteen females, data which would seem to indicate that the hair of the scalp, even in female infants, acknowledges a sexual influence. Alterations of the nails are reported rather less often than changes in the teeth, but for reasons named above the conclusions are not trustworthy.
From the observations heretofore published, it is made clear, however, that the absence of hair may be limited to one, several, or all regions of the body, including the scalp, brows, beard, axillæ, pubes, and the surface normally covered with lanugo. The “complete and absolute” cases, of the sort described by Eshner, Schede and Ziegler, as also that of the negro photographed for Crocker. are extreme divergencies from the average and may be due either to non-development of the hair-pouches or to the intra-uterine atrophy assumed by some authors to explain the result. The Australian races described as hairless seem to be groups of aborigines of that country, only some members of which are completely destitute of hair. It is worthy of note that among the cases on record there are not a few subjects of the anomaly in [p.35] whom there has been improvement of the condition of the hair under an appropriate therapy.
In the records of congenital alopecia, individuals are cited, not only of one family, but of generations of a single family, who have been similarly affected. I have published the details of the case of a female child, six and one half years of age, being the third of six children affected with hypotrichiasis. In not a few instances, father and child, mother and child, maternal grandmother and uncle, cousins-german, and other near or but slightly removed relatives of the subjects of the anomaly, have exhibited both natal and post-natal hypotrichiasis. Notable in this connection is the history detailed by Nicolle and Halipré, where congenital alopecia affected in six generations thirty-six individuals. It is clear, how- ever, not merely from the family history described, but also from others on record, that atrichia and hypotrichia, in various grades, may affect one individual where no evidence exists that any other member of the family for generations has similarly suffered.
Apparently the most common of coincident anomalies, in cases of congenital alopecia, are changes in the teeth and nails. Kings- bury calls attention to a possible connection between the normal dehiscence of the long hair of the infant at birth, and the fall of the milk teeth, as if both processes were obedient to one law. In some of the lower vertebrata, certain kinds of fishes for example, the teeth are shed in a succession as regular as that observed in human hair.
When defects of pilary development in the human family are noted at birth, the teeth which are erupted later may be changed in gradations from the condition in which few, defective, oddly arranged or shaped, or doubly ranked teeth are developed, to the point of complete edentulism. It is interesting to note that when but three or four teeth are reported as present, these are usually molars or pre-molars of the lower jaw, the incisors and canines being often absent. The stress of reversion seems to be first declared in the organs earliest to develop under normal conditions. If this be the law, it holds good only for organs originating from the epiblast, as the reverse seems to be the rule when the mesoblast has participated in the genesis of the part. In several types of edentulism, as in the subjects of defect of hair at birth, a family predisposition to such anomalies can often be determined.
[p.36] Other abnormal conditions associated with atrichia and hypo- trichiasis are found in those who have abolished or defective secretions; who do not sweat; who shed no tears; who have absence of or impaired sense of smell and taste; and who are not provided with mammary glands. In a case of congenital hypotrichosis, Ziegler found blind sebaceous and coil-gland ducts with arrector-pili muscles but no hair-papillæ.
The most of the subjects of this anomaly seem to have been exempt from inflammatory changes in the tissues which depart from the normal in any region of the body. It is recorded in a few observations that onychitis and infective processes of the nail had been recognized: in others a progressive atrophy of the scalp and nail-matrix had occurred. Both the subjects of the anomaly and their progenitors are repeatedly reported as the victims of alopecia areata, and this with recurrent attacks. Wende’s patient had atrophy of the finger-tips and hereditary epidermolysis bullosa: Guilford’s and Luce’s suffered from xeroderma: Aubry’s from an hydrocephalus, the consequent disorder having been attributed to the pressure along the fontanelles.
Anomalies of the eyes are apparently among the rarest of phenomena associated with natal and post-natal hair-defect. Eshner reports the case of a man sixty-four years of age, who after birth had been hairless in all parts of the body, the nails of whose fingers and toes were faultily developed and transversally ridged. In this case there were numerous mosaic-like areas of whitish masses in the retina, believed to be a consequence of retinitis albicans. The teeth were presumably involved, though the age of the subject and a history of some fallen teeth made the dental history obscure. MacNoughton Jones and Ringrose Atkins report the case of a boy who never had had more than a light down on the face and the region of the beard. The teeth were ridged, discolored, and sepa- rated; the finger-nails were aborted and furrowed. The patient suffered from disorder of the eyes. In June, 1905, a female child of Jewish parentage, three years of age, was brought to me from Michigan whose case falls in the second category of the class de- scribed above, and in the first of the variations named. At birth, the scalp of this child had been covered with normal hair. In one month this fell, leaving a completely denuded surface which had never since been the seat of a pilary growth. On examination the [p.37] scalp was found to be smooth, firm, glistening and destitute of hair save over two or three points where downy filaments could be recognized with a lens. The nails of the hands and feet were seriously changed, being both ridged and discolored. Dr. Harper, of Chicago, was good enough to examine the eyes of this patient for me and he reported the presence of opaque patches in the retina. There was no history of family anomalies. One child of the same parents had died of nasal hæmorrhage. Dr. Winfield’s patient evidently suffered from some visual defect.
These four cases and one which is referred to later in this contribution to the general subject (a record of ocular symptoms co-existing with polydactylism), though few in number, challenge enquiry. The hypothesis that the retinal patches recognized in Eshner’s cases and mine were due to a pre-existing inflammatory process, seems less reasonable than the possibility that the ocular globes shared in the diversion from type, recognized in the scalp and hands. I am indebted to Dr. Casey A. Wood for the suggestion that the retinal plaques recognized in these cases are “brushes,” or areas of opaque nerve fibre, seeing that in the lower mammalia this condition is not only exceedingly common but normal. fishes, birds, and the lower mammals, the opaque nerve fibres are exhibited in white or whitish areas, or in feathery distributions, or in other forms none of which occur in the normal eye of man. Is there not here, as in hypotrichiasis and edentulism, a reversion to the type of the mammal leading in part a sub-aqueous existence, whose eyes as is well known, are designed for vision beneath the surface of water, and therefore are provided with a thickened sclerotica projected forward along the orbital axis with the retinal tissue proportionately reduced?
According to Prof. Owen, in the descent from the higher to the lower type of mammalia, the thumb and great toe gradually become rudimentary, and the little finger and little toe unimportant with respect to the chief function of both fore and hind extremities; while next in order of importance are ranged the second and fourth digits. In comparative anatomy, the primacy of the hand and foot rests with the middle finger and middle toe, their adjuvants projected on either side. For example, the horse, as all anatomists know, walks on his third finger and third toe; the ox on a combi- nation of the third and fourth. In the foot shown in the photo- [p.38] graph, a distinct reversion to type is betrayed in the relative shortness of the big toe and the marked projection of the member composed of the fused second and third toes which furnishes the chief support of the foot in advance of the line of metatarsals.
It is an interesting fact of pathology that divergence from the normal, in the direction of both excess and defect, may be coincident or successive. The deeply pigmented skin of the negro most often furnishes the pure type of the albino; in both sexes hypertrichosis of the face is often coincident with forms of alopecia of the hairy scalp; Kingsbury calls attention to the fact that general hirsuteness may be accompanied by defective dentition; and similarly the subjects of syndactylism may also exhibit polydactylism in various types. Here also, in certain cases, a family predisposition to such defects can be recognized. A female child was shown to me in June of the current year having a rudimentary sixth digit on each hand and foot, the father and grandfather being reported as similarly departing from the normal.
After a somewhat careful search I have been unable to discover reference to cases, save as here reported, of co-existence of con- genital alopecia with syndactylism. In the voluminous literature accumulated on the subject of syndactylism and polydactylism, it is apparent, first, that the two deformities frequently co-exist in one individual; second, that the larger number of contributors have been concerned chiefly with the surgical management of the webs and of the supernumerary digits. When there is co-existence of structural anomalies, as a rule only those organs are involved which comparative embryology has demonstrated to be related in their genesis. Yet Parham reports a case of polydactylism in which there were coincident changes in the pupil. Apparently no ophthalmoscopic examination was made. There was also absence of testes, hypospadias, and thickening of the maxillary bones. On the other hand it is noteworthy that the general health of most of the subjects of congenital alopecia is unimpaired. The genital organs, as in the subject of the anomalies here reported, are commonly not abnormal. Atkinson’s patient, destitute of the sense of smell and taste, was completely edentulous, yet was the father of eight children, two of them edentulous girls. S. H. Guilford’s patient, forty-eight years of age, had a scalp covered with fine down, no teeth, defective smell and taste, did not sweat, and was the father of eight children, [p.39] some edentulous. Beauvais, Rayer’s patient, is said to have contracted syphilis twice.
Respecting the grade of syndactylism shown in the photograph, the webs seen in the hand are less extensive than those uniting the digits of the feet, though in both sets of organs these were firmer and more voluminous than in many cases of syndactylism where the uniting membrane is thin and composed chiefly of the elements of the epidermis. In the present case, the webbing of the toes was sufficient to produce a firm fusion of the attached digits.
Aside from the abnormal features enumerated, it may be set down that the thyroid enlargement in this case was scarcely sufficient to constitute a distinctly morbid symptom in a young subject at the puberal epoch. The separated, pointed and relatively small-sized teeth were, however, as in Winfield’s patient, significant. The bone tumor of the calcaneum seemed to be limited to one side of the body. Skiagraphic observation of the corresponding foot gave negative results.
The group of congenital anomalies represented by nævi of various types, by ichthyotic and other cutaneous keratoses, by verrucous lesions, and by alterations of the hair, nails, and teeth, are obviously developmental diversions from the normal, originating in structures derived from the epiblast of the germinal cell mem- brane. Few of them are of a character sufficient to threaten life or seriously to interfere with much else than cosmetic conditions. Whether these, all or singular, are in the line of a reversion to a lower type of organism as the result of a purely aberrant or de- generative process, is not difficult to determine. The so-called “freaks of nature” collected in pathological museums and represented in the experience of clinicians, are not diversions at random from the type of normal genesis and growth, but are known to obey laws as definitely formulated as those regulating karyokinesis and phagocytosis.
While the structures derived from the epiblast of the blastosphere, the hair, nails, and organs of special sense, are those chiefly concerned in the anomalies coincident at birth with hair-defect, a fact to be considered as of importance in this connection is that both the epiblast and the mesoblast concur in some of the evolutionary processes of the body; as, for example, when the extremities first bud as outgrowths from the lateral parts of the embryo, the [p.40] muscular and skeletal structures being thus developed. In most of the animals furnished with articulated extremities, the forelimbs are produced before the hind. This possibly explains, in such anomalies as those under discussion, the incomplete degree of webbing of the fingers as contrasted with the well nigh complete union of some of the digits of the feet, the point of time of developmental interference, if such a term be permissible, determining the grade of the deformity. Syndactylism is much more common in the feet than in the hands. In other words, within certain limits, the later the divergence from the normal, the greater the chance that the organs derived from the epiblast and mesoblast will be involved; and, given the co-operation of the two in the evolution of the body, the anterior extremities will presumably be more fully developed and more exempt from anomaly than the posterior.
Comparative embryologists are not yet in agreement as to whether the pentadactyloid limb is derived from the piscine fin, but there are strong arguments in favor of such a position. During its placental relations, the human foetus leads an exclusively sub- aqueous existence. No violence is done to the laws of embryonic development, whether normal or perverted, in viewing the co-existence of the group of anomalies herein considered, as a reversion to type of some partially aquatic animal. The primordial unit should have been found among the amphibious mammalia, and have been provided with an integument either covered with scales or with short, stiff hairs; should have seized its prey with a few pointed incisor and molar teeth, the latter at least to the number of three or four in the lower jaw, though these may have been wholly wanting; and should have propelled itself, whether on water or land, with fully webbed pentadactyloid paws on the hind limbs, these organs having been developed originally from the piscine fin.
DISCUSSION.
DR. JAMES MACFARLANE WINFIELD said the case reported by Dr. Hyde reminded him of a similar one that had come under his observation about seven years ago. The patient was a man about 35 years old who had not a congenital alopecia, but a congenital thinning of the hair. His hair did not begin to grow until he was a child of 5 or 6. The pubic and axillary hairs were thin, straggling and silky, his skin was dry and coarse. In addition, the patient was [p.41] very near-sighted. The doctor considered these cases to be examples of degeneration, and was under the impression that they were due to ancestoral syphilis.
DR. GROVER W. WENDE said that Dr. Hyde, in collecting cases showing the association of all kinds of congenital alopecia with different pathological conditions, conferred a favor upon dermatologists. Some years ago he had reported two instances of congenital alopecia associated with epidermolysis bullosa hereditaria, which might appropriately be included in Dr. Hyde’s classification. The special influence of epidermolysis bullosa hereditaria in connection with the peculiar changes in the skin, as well as the delayed development of hair, both may be traced to the same cause. One of the later cases showed atrophy of the finger-ends – a like case had been reported by Dr. Stelwagon, in which the atrophy was more marked; but his patient was much older, and there were no hair-changes. All these conditions may be due to one and the same cause their origin may be embryonic.
DR. A. RAVOGLI asked Dr. Hyde if in the case he reported he had found any connection with hereditary syphilis. Personally, he could recall one or two cases of that affection associated not with complete baldness, but with a very scanty growth of hair, and, in one case, with imperfect development of the fingers. One of the cases died of meningitis at the age of five.
DR. W. A. PUSEY asked if the influence of consanguinity in marriage was apparent in any of these cases.
DR. HYDE, in closing, said that in the case he reported there was no evidence or suspicion of hereditary syphilis or no consanguinity in marriage. The family history was remarkably good. While there was an enormous bibliography in connection with this general subject, cases of congenital alopecia, judging by the records, were relatively rare. Among 277 cases of syndactylism reported by Gaston Roblow, no reference is made to an associated alopecia. In fact he would not have reported his case in detail were it not for the fact of its rarity, as appears from a careful search of literature.
PARTIAL BIBLIOGRAPHY.
(ALOPECIA CONGENITAL)
CROCKER, H. Radcliffe, “Dis. of the Skin,” 3rd Edition, 1903, 1200 Atlas, Plate XC, Fig. 13.
GOULD: “Anomalies and Curios. of Med.,” 1897, p. 226.
[p.42] SCHEDE, M.: Arch. f. klin. Chir., Bd. XIV, 1872, pp. 150-158. Study of sections of Scalp.
ZIEGLER, P.: Arch f. Derm. u. Syph., Bd. XXXIX, 1897, p. 213.
THURNAM, J.: Med-Chir. Tr., LIX, 1886, p. 473 and 1848, XXXI, p. 71.
HUTCHINSON, J.: Med.-Chir. Tr., 1886, LXIX, p. 475; Lancet, 1886, Vol. 1, p. 293.
MOLENES DE P.: Annal de Derm. et Syph., Vol. 1, 1890, p. 548.
PINKUS, F.: Arch. f. Derm. u. Syph., Vol. 1, 1899, p. 347. (With full biography.)
AUDRY: Jour. des mal. Cut. et. Syph., XIV, 1902, p. 9. Ibid. 1900, p. 161; Ann. de Derm. et Syph., 1893, p. 899.
WHITE, C. J.: Jour. of Cutan. and Gen.-Urin. Dis., XIV, 1896.
SEDGWICK, Wм.: Brit. and Foreign Med. Chir. Review, 1863, Vol. XXXI.
HYDE, J. N.: Intern. Clinics, Philadelphia, April, 1891, p. 321.
TEVEN-ELFERFREED: Monats. f. Prakt. Derm., 1902, XXXV, p. 149.
HILL, J. HIGHAM: Brit. Med. Journ., 1881, Vol. 1, p. 177.
Fox, G. H.: Journ. of Cutan. Dis., 1902, Vol. XX, p. 1.
WILLIAMS: London Med. Gaz., 1848, Vol. VI, p. 337.
Pernet, Geo.: Brit. Journ. of Derm., 1900, p. 100.
Darier et Le SOURD: (Brocq in Discussion) Annal de Derm. et de Syph., November, 1898.
GILFORD HASTINGS: Practitioner, August, 1904, p. 188.
AUBRY: Ann. de Derm. et Syph., 1893, 3 ser., tome IV, p. 899.
WENDE, G. W.: Journ. of Cutan. Dis., 1904, XXII, p. 14, Plate V, Three Photographs.
KINGSBURY, J.: Journ. of Cutan. Dis., 1906, XXIV, p. 419; Bibliography and two photographs, one representing sections of scalp.
SINGER: Unser. bisher. Kenntniss d. angebor. Haarlosigkeit; Inaug. Th. Erlangen. KRAUS: Arch. f. Derm. u. Syph., 1903, LXVI, p. 369.
ESHNER, A. A.: Amer. Journ. of Med. Science, April, 1905, with bibliography.
NICOLLE ET HALIPRE: Ann. de Derm. et de Syph., 1895, Vol. VI, pp. 675 and 804.
RAYER: Skin Diseases, Berlin, 1839. Theoret. and Pract. Treatise on Dis. of the Skin, 2nd Edition, Translated by R. Willis, London, 1835, 1049.
FORDYCE, J. A.: Journ. of Cutan. and Gen. Urin. Dis., March, 1895. ABRAHAM: Brit. Med. Journ., April, 1895, p. 814.
BRANDT, ALEX.: Biolog. Centralb., March 1, 1897, Bd. XVII, p. 161.
MICHELSON, PAUL: Handbuch der Hautkrankheiten in Ziemssen’s; Handbuch der speciellen Pathol. und Therapie, Leipzig, 1883, p. 107.
STEIMIG: Notizen aus dem Gebiete der Natur-und Heilkunde, Bd. XXVI, No. 4, Nov., 1829, No. 554, p. 50.
SOUTH, JOHN F.: Transl. of Adolph Wilhelm Otto’s Compendium of Human and Comparative Pathological Anatomy, London, 1831, p. 120.
EBLE, BURKARD: Die Lehre von den Haaren in den gesammten organischen Natur, Wien, 1831, Bd., 11, p. 224.
HEISTER, LAURENT: Med. Chir.und Anat. Wahrnehmungen, Rostock, 1753.
WELLS, W. C.: Trans. of a Society for the Improvement of Medical and Surgical Knowledge, 1900, Vol. 11, p. 213.
BETTMAN: Arch. f. derm. u Syph., LX, p. 343, 1902.
LUCE: Schmidt’s Jahrb., Bd., CXCI, Heft. 1, p. 31.
QUILFORD: Wien. Med. Woch., 1883, No. 37, p. 1116.
JONES AND ATKINS; Dublin Journ. Med. Sci., 1875, Vol. IX, p. 200.
MIELUCHO-MACLEAY: Zeits f. Ethnol., XIII, 1881.
ALOPECIAS ASSOCIATED WITH DENTAL CHANGES:
LAUMONIER: Rev. d’Ondontolog., Paris, 1905, XXIV, p. 490.
[p.43] JEAN: Pelade d’origin. Dent; Bull et Mem. Soc. de Méd. d. Vauclause, 1905-6, 1-11, p. 317.
ALLAEYS: Pelade d’origin. Dent, Rev. Trimest. Suisse d’Ondontol, 1906. XVI, p. 1.
PATTE, ED.: Essai, Paris, 1904, No. 202.
DELGUEL: Gaz. Ibshd. d. Sci. Med., Oct. 28, 1906.
COMPARATIVE EMBRYOLOGY, SYNDACTYLISM, and POLYDACTYLISM:
BALFOUR: Comp. Embryology, London, 1886, p. 394, Vol. 1.
BROCA: La Syndactylisme Congénitale. Study of 277 cases by Gaston Roblot, Thèse de Paris, 1906.
PARHAM, F. W.: New Orleans Med. and Surg. Journ., 1887, 755.
BOWEN, JOHN T.: The Epitrichial Layer of the Epidermis. J. Cut. Dis., 1895; XIII, 485.
OHMANN-DUMESNIL: Teratologia, July, 1895, 11, 3, p. 149.
ANDERSON, W.: Deformities, etc., London, 1897.
BENO, J.: Essai sur la syndactyl. congénitale, Monog., 1886, Nancy, No. 238.
LEVIN, E. G.: Berlin, 1895.
MESSERSCHMIDT, Greifswald, 1885.
DUBREUILH and PETGES: Annal. de Derm. et de Syph., 1908, 5, 17.
LANGLET: Annales, 1903, IV, 369.